When experiencing tightness in the back of your legs, it’s common to assume it’s due to tight hamstrings. However, nerve tension, particularly involving the sciatic nerve, is often mistaken for muscle tightness. Understanding the distinction between nerve and muscle issues is crucial for effective treatment.
The Difference Between Nerves and Muscles
Muscles are elastic tissues responsible for movement and maintaining posture, while nerves are part of the nervous system, transmitting signals between the brain and the body. When muscles are tight, they limit flexibility and strength, requiring prolonged stretching to lengthen them. Nerves, however, are non-elastic, and prolonged stretching can irritate them, leading to increased tension. This is why it’s crucial to determine whether your tightness is due to muscle or nerve tension.
Sciatic Nerve vs. Hamstring Tightness
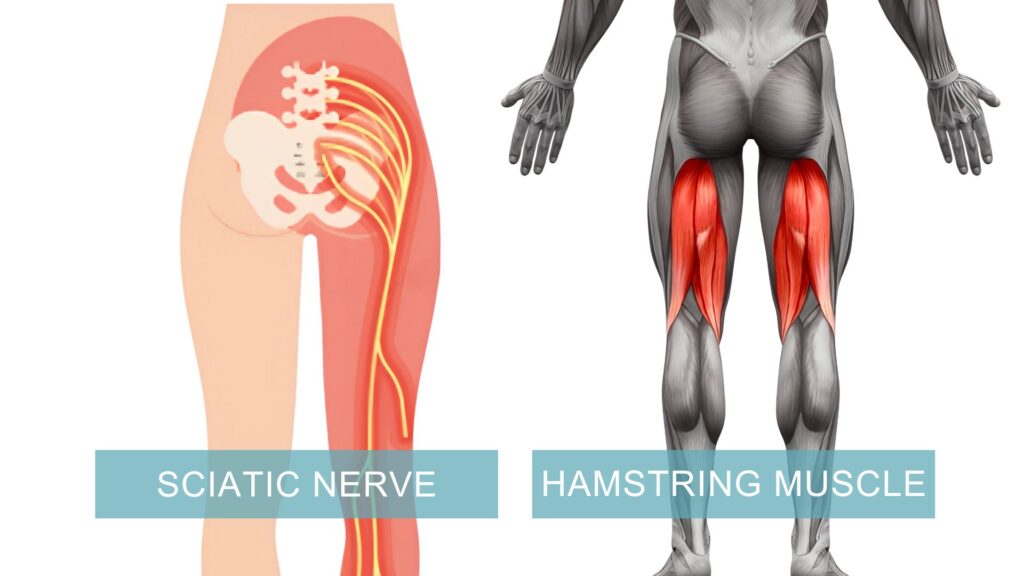
The sciatic nerve runs from the lower back through the hips and down each leg. When this nerve is compressed or irritated, it can mimic hamstring tightness. Key differences include:
- Hamstring tightness: Typically involves a restricted range of motion when stretching the back of the leg, with a deep pulling sensation in the location of the muscle (behind the thigh).
- Sciatic nerve tension: May involve a sharper, burning pain, numbness, tingling, or tight sensation that can extend beyond the hamstring, often down the leg and into the foot.
Symptoms of Excess Nerve Tension
Signs that you might be dealing with nerve tension include:
- Persistent muscle tightness in the hips and lower legs, unrelieved by stretching.
- Pain that comes and goes, often sharp or burning in nature.
- Numbness or tingling sensations in the legs or feet.

Causes of Nerve Tension
Several factors can contribute to nerve tension, including:
- Decreased Spinal Mobility: Limited movement in the spine can compress nerves.
- Poor Sitting Posture: Slouching or sitting for prolonged periods can strain the sciatic nerve.
- Poor Walking Posture: Standing and walking with an incorrect spinal curve can irritate the sciatic nerve over time.
- Tight Back Muscles: Muscle imbalances or tension in the lower back can put pressure on the nerves.
The Importance of Accurate Diagnosis
Since the treatment for nerve tension and muscle tightness differs significantly, identifying the correct issue is essential. Stretching exercises that benefit tight hamstrings might aggravate nerve tension. Conversely, nerve glides designed to alleviate nerve tension won’t effectively address muscle tightness. Accurate diagnosis ensures you receive the appropriate interventions for relief and recovery.
Broader Implications of Nerve Tension
This concept isn’t limited to the lower body; it also applies to other areas, including the upper extremities. Nerve tension in the arms or hands can mimic muscle tightness or strain. A physical therapist can assess these areas to determine whether nerve tension is contributing to your symptoms and provide appropriate treatment.
When to See a Physical Therapist
If you suspect nerve tension, consider consulting a physical therapist. They can provide a precise diagnosis and develop a tailored treatment plan. Addressing nerve tension early can prevent discomfort from becoming a more significant issue. A physical therapist can help you understand the underlying causes and guide you through effective strategies to alleviate your symptoms and improve overall mobility.
Understanding the difference between nerve tension and muscle tightness is key to effective treatment and recovery. If you’re unsure about the source of your discomfort, seeking professional advice can help you find the right path to relief.
References:
Giuffre, B. A., Black, A. C., & Jeanmonod, R. (2023). Anatomy, Sciatic Nerve. StatPearls. StatPearls Publishing. Retrieved from https://www.ncbi.nlm.nih.gov/books/NBK482431/
Mayo Clinic. (2024). Sciatica – Symptoms and causes. Mayo Clinic. Retrieved from https://www.mayoclinic.org/diseases-conditions/sciatica/symptoms-causes/syc-20377435
Cleveland Clinic. (2018). Hamstring muscles: Location, anatomy & function. Cleveland Clinic. Retrieved from https://my.clevelandclinic.org/health/body/21904-hamstring-muscles